View Larger Image

Stephenson and his wife, Brittany, visit UAMS for a checkup.
Patient Uses FaceTime to Call Family During Brain Surgery
| Before his seizure on May 31, 2018, Chris Stephenson, of Horatio, Ark., had no idea he had a tumor the size of an orange in his brain. He was logging about 4,000 miles a week in his big rig and happened to be driving when the seizure happened.
“It took four paramedics to get me out of the truck,” Stephenson said. “I was in Chicago and they took me to a hospital there. I had an MRI and that’s where they saw the growth.”
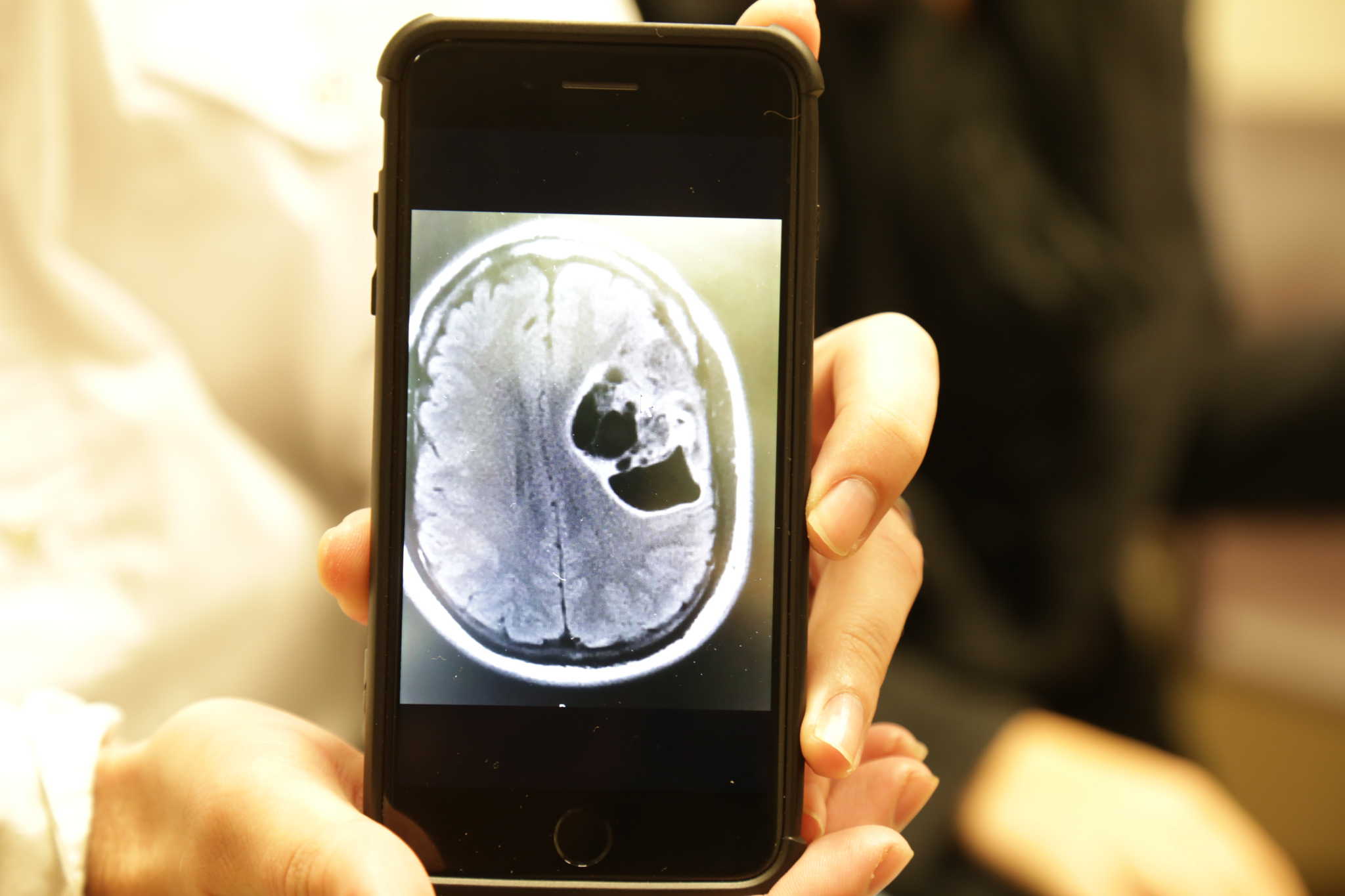
Chris Stephenson’s brain tumor was about the size of an orange. He keeps an image of the scan on his phone.
Stephenson eventually made his way to UAMS where a second MRI confirmed the growth was malignant. J.D. Day, M.D., professor and chair of the UAMS Department of Neurosurgery would have to open his skull to remove the tumor.
“It was a lot to take in. But I wanted to stay strong for my family and prepare myself for whatever happened.”
What happened next was a first for UAMS and possibly a first for neurosurgery anywhere: Stephenson and his family got a little help from their phones.
Indranil Chakraborty, M.D., is an associate professor and director of the Division of Neuroanesthesiology at UAMS. Because of the tumor’s location, Stephenson would have to be awake during the surgery so that Day could monitor Stephenson’s brain activity to make sure they were not damaging his speech and motor skills.

Indranil Chakraborty, M.D., director of the Division of Neuroanesthesiology at UAMS.
UAMS has been doing awake craniotomies since 2014. Chakraborty has established a procedure to ensure success with each of the patients. He says it’s not uncommon for even the most prepared patient to experience a little anxiety. In thinking of additional ways the operating room staff could make the patient comfortable, Chakraborty presented the idea of using FaceTime, a capability that allows a person to video chat with another person through each of their phones.
“I was ready to hand over my phone as soon as he mentioned it,” said Brittany Stephenson, Chris Stephenson’s wife.
The first time she received a call from the operating room, she says she couldn’t make out much more than blue drapes.

Chief neurosurgery resident, Heather Pinckard-Dover, M.D., dials Brittany Stephenson for a FaceTime conversation in the operating room.
“The second time they called, it was nice,” she said. “We were able to talk to him and he sounded calm. It felt better to hear straight from him. He was telling jokes and seemed to be doing very well.”
She received three calls in all from the operating room. The surgery took about six hours.
In addition to being able to monitor a patient’s brain activity, Chakraborty says awake craniotomies benefit the patient because they’re in less pain after the surgery. Patients are also able to eat and drink sooner, and in many cases they go home earlier than patients who were under general anesthesia in a craniotomy.
Stephenson’s case was the first time in Arkansas that a patient has been able to video chat with family during an operation. Chakraborty has neuroanesthesiology colleagues around the world and says none of them have heard of video chatting happening anywhere else at the time of Stephenson’s surgery.
“It is definitely an innovative way to demonstrate patient- and family-centered care,” Chakraborty said.
Because this form of communication has been so well-received, neurosurgeons have since used video chat twice more in the operating room.