
Simulation Immerses Nursing Students in Details of the Operating Room
| About a dozen nurses gathered around a patient strapped to a table in a cold operating room. In the background sat an intubation laryngoscope, anesthesia machine, sonogram equipment and cabinets full of bandages, tape, clamps, alcohol wipes, equipment, and other necessities found in any operating room.
Four at a time, the nurses listened together through the same stethoscope for distinct characteristics of irregular breathing, such as crackling, wheezing and whether it sounded wet or coarse.

A crash cart filled with an array of medications, represented by distilled water, organized as they would be in the operating room.
However, the nurses were actually students and the patient was a $50,000 high-fidelity manikin, complete with some internal organs, pulses, pupil dilation, the ability to breathe, and countless other bodily functions all controlled by a computer. The operating room itself was a new simulation area set up in the Innovative Practice Center (IPC) of the UAMS College of Nursing.
While the primary purpose of the IPC operating room is to serve as a training ground for the nurse anesthetist program, which is undergoing accreditation, it also serves as a nonthreatening introduction to the operating theater for all Bachelor of Science in Nursing students.
“We created a new world in here, a new setting in which we can take our learners from the very simple to the very complex,” said Pam deGravelles, Ph.D., RN, IPC/ simulation coordinator and a clinical assistant professor. “Once they get comfortable with this area, we can go down to the UAMS Simulation Center where a more advanced operating room will take them into even more complex situations and really ramp it up. But this is where we’re going to start their training and education on the principles of OR nursing.”
That training involves students being able to react in real time to programs installed within the software for the manikin, named HAL. While the medication vials on hand are filled with only distilled water, instructors can program the simulated patient to react to injections, increasing heart rate, slowing breathing, lapsing into incoherent speech or even dying.
“This suite is also a simulation theater with two mounted cameras on the ceiling and wall. We can record scenarios and play them back to learn from them or broadcast them to a classroom for student and faculty observation,” said deGravelles. “Simulation is meant to be a safe learning environment, after which we will debrief for at least twice as long as we’re in the simulation so students can gain a deeper understanding to build safer behaviors to increase patient safety and outcomes.”
“Everyone can watch and learn, evaluating each action in advance so that we make the best decisions when faced with real patient encounters. These learning opportunities are priceless,” she said.
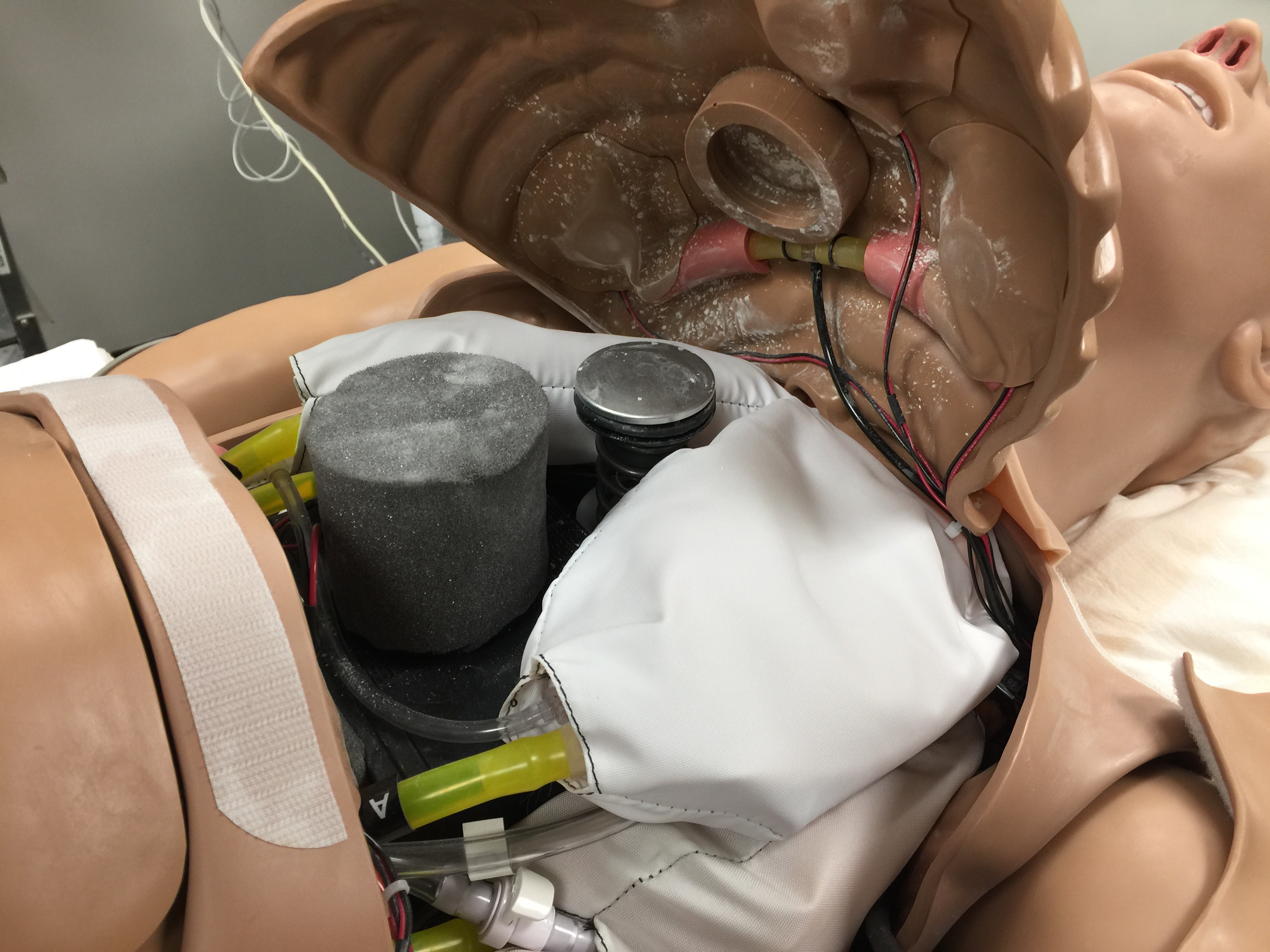
HAL, a high-fidelity manikin, is filled with electronics and sensors to replicate the vitals of a real patient.
It is a very different and far more realistic way of training than only a few years ago, said Michelle Gonzalez, Ph.D., CRNA, director of the forthcoming nurse anesthetist program. Training in a simulated operating room environment is a vital part of education and training of nurse anesthetists, as a majority of their professional life will be spent in operating room settings.
“We couldn’t provide a high-quality education without this type of realism in the learning environment” she said.
Pointing to the anesthesia station, which is an actual, working machine pulled from an operating room, she explained how it was set up so that students could easily learn the process of selecting and setting up the appropriate equipment, the right drugs, drawing them into the correct syringe and labeling them appropriately, all while cross checking to make sure it’s the right combination for the patient on the table.
It’s a process that might take 45 minutes in the early days of learning, but gets down to 10 minutes with practice and repetition. And that’s why simulation is needed, “ultimately it leads to a higher degree of safety for patients once the student begins clinical practice”
Gonzalez noted the goal in putting together the simulated operating room has been to make it useful for all levels of nursing education. Although the majority of equipment in the operating room is specific to anesthesia care, there are opportunities to use the equipment to foster partnerships across programs in the College of Nursing and with the UAMS Simulation Center.
Pulling over the Glide Scope and demonstrating how it’s used for intubation, she said it’s not something students would operate without advanced practice. But just knowing what it is and how it works, even as an undergraduate student, will make for better prepared operating room nurses.
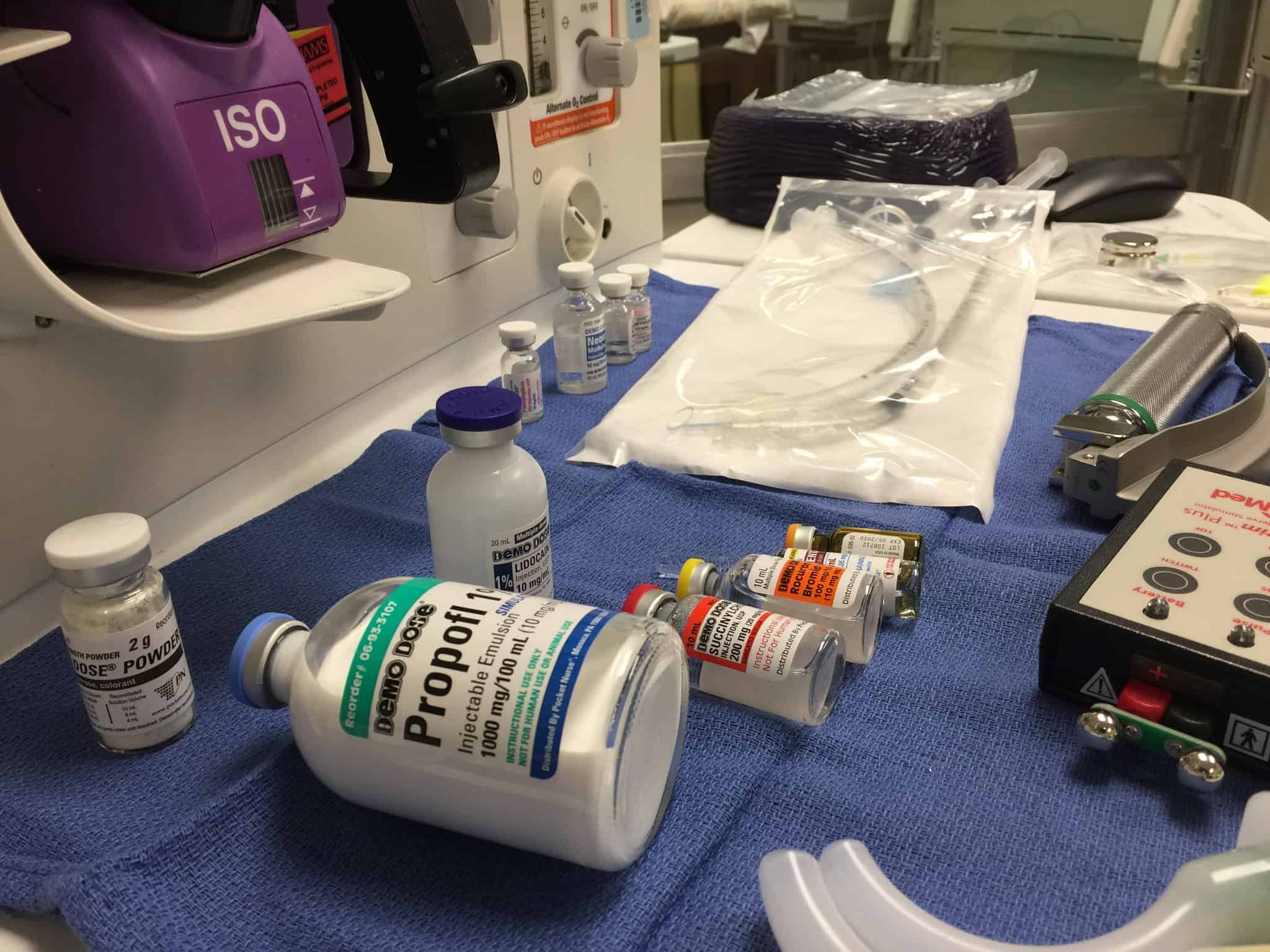
Simulated medications laid out on the anesthesia machine are clearly labeled and intentionally misspelled.
“They may get asked if a particular tool is available or ready, and they don’t have to ask what that is or go looking for it,” she said. “They know what to look for. They’ve seen it and know how it’s used. They’ll potentially become more comfortable with the equipment and in their work settings.”
That’s the reason for the level of detail in the simulated operating room, right down to the labels on the vials of medication. They’re clearly marked for instruction purposes only and the names are intentionally misspelled (Propofl instead of Propofol), but the packaging, size and placement are all where one would expect in a real clinical setting.
“We want to have this be as authentic a learning setting as possible for our students,” said deGravelles. “That’s the reason we created it.”